
|
|
“Gaon Swasthya Samikhya”1- A Process to Foster Community Action in Odisha, India
|
Sudarshan Das
|

Introduction
Community monitoring of health services is the “systematic documentation and review of the availability, accessibility and quality of health services against specific government commitments or standards by actual beneficiaries of services, for the purpose of doing advocacy with service providers and policy makers to improve the services.
Public health is the practice of preventing disease and promoting good health among the people, from small communities to the entire country. The public health system in India comprises a set of state funded and managed health care facilities. Community participation is expected to be a key component of the public health system. The declaration of Alma-Ata states: “Primary health care... requires and promotes maximum community and individual self reliance and participation in the planning, organisation, operation and control of primary health care, making fullest use of local, national and other available resources; and to this end develops through appropriate education the ability of communities to participate” (Para VII (5), Alma Ata Declaration, 1978).
The vision statement of the National Rural Health Mission (NRHM)2 has stated one of its goals as “To set up a platform for involving the Panchayati Raj Institutions3 and community in the management of primary health programmes and infrastructure”. The section on the core strategy of the mission of the NRHM states, “If the mission of health for all is to succeed, the reform process would have to touch every village and every health facility. Clearly it would be possible only when the community is sufficiently empowered to take leadership in health matters”. Therefore, the participation of PRI members, service providers and community is essential for community based monitoring or community based action in NRHM as a rights platform.
Community monitoring of health services is the “systematic documentation and review of the availability, accessibility and quality of health services against specific government commitments or standards by actual beneficiaries of services, for the purpose of doing advocacy with service providers and policy makers to improve the services.
Public health is the practice of preventing disease and promoting good health among the people, from small communities to the entire country. The public health system in India comprises a set of state funded and managed health care facilities. Community participation is expected to be a key component of the public health system. The declaration of Alma-Ata states: “Primary health care... requires and promotes maximum community and individual self reliance and participation in the planning, organisation, operation and control of primary health care, making fullest use of local, national and other available resources; and to this end develops through appropriate education the ability of communities to participate” (Para VII (5), Alma Ata Declaration, 1978).
The vision statement of the National Rural Health Mission (NRHM)2 has stated one of its goals as “To set up a platform for involving the Panchayati Raj Institutions3 and community in the management of primary health programmes and infrastructure”. The section on the core strategy of the mission of the NRHM states, “If the mission of health for all is to succeed, the reform process would have to touch every village and every health facility. Clearly it would be possible only when the community is sufficiently empowered to take leadership in health matters”. Therefore, the participation of PRI members, service providers and community is essential for community based monitoring or community based action in NRHM as a rights platform.
Community monitoring of health services is the “systematic documentation and review of the availability, accessibility and quality of health services against specific government commitments or standards by actual beneficiaries of services, for the purpose of doing advocacy with service providers and policy makers to improve the services.
|
NRHM has emphasised on community based monitoring which includes not only engaging community in monitoring of health services but also planning and implementation of the schemes that promote good health of the people. This process is not considered as a fault finding but a fact finding mechanism and promotes good understanding between community and service providers for better outcome of the health care services. Community monitoring is also a mechanism for ensuring greater government accountability and transparency in health care to its citizens at the local, regional and national levels. The community based monitoring (CBM) process was first initiated as a pilot in nine states of the country including Odisha.
|

|
Background and Perspectives on Community Action in Odisha Drawing the mandate from the NRHM framework, Odisha
The term community monitoring had been changed to community action during the course of implementation of Phase-I project to involve all stakeholders and for imbibing a shared perspective of fact finding rather than fault finding for improved planning and implementation of the health programmes in the community.
Drawing the mandate from the NRHM framework, Odisha was one of the nine states to implement the first phase of community monitoring in four districts (namely Bolangir, Kendrapada, Mayurbhanj and Nabrangpur) in the year 2006-08.
After successful completion of the first phase of community action in Odisha it was planned that the state government will take the ownership of the process and upscale/ further expand the programme from its own budget supported under this programme implementation plan (PIP) with the support of State Advisory Group on Community Action (SAGCA). Proposals were submitted to the Mission Director in 2008 to extend the community action programme covering all villages and blocks in the four districts where the process has been initiated in the first phase. However, the state government felt that there was a need for a change in the community monitoring tools considering the complexities and level of literacy among the members of the community in the state giving the process a setback. the complexities and level of literacy among the members of the community in the state giving the process a setback.
The initial enthusiasm during the phase one among the key stakeholders and the SAGCA was lost as it was felt that the process may not be sustainable without government ownership and support. However, with the change of leadership at the Mission Directorate level in 2010, the efforts of SAGCA regained momentum.
1. Gaon Swashtya Samikhya is an expression in the Odiya language which loosely translates to Village Health Review.
2. NRHM is a common platform for delivery of public health services in rural India.
3. The Panchayati Raj Institutions or PRI are the local self government institutions at the village, subdistrict and district levels comprising of locally elected representatives.
The term community monitoring had been changed to community action during the course of implementation of Phase-I project to involve all stakeholders and for imbibing a shared perspective of fact finding rather than fault finding for improved planning and implementation of the health programmes in the community.
Drawing the mandate from the NRHM framework, Odisha was one of the nine states to implement the first phase of community monitoring in four districts (namely Bolangir, Kendrapada, Mayurbhanj and Nabrangpur) in the year 2006-08.
After successful completion of the first phase of community action in Odisha it was planned that the state government will take the ownership of the process and upscale/ further expand the programme from its own budget supported under this programme implementation plan (PIP) with the support of State Advisory Group on Community Action (SAGCA). Proposals were submitted to the Mission Director in 2008 to extend the community action programme covering all villages and blocks in the four districts where the process has been initiated in the first phase. However, the state government felt that there was a need for a change in the community monitoring tools considering the complexities and level of literacy among the members of the community in the state giving the process a setback. the complexities and level of literacy among the members of the community in the state giving the process a setback.
The initial enthusiasm during the phase one among the key stakeholders and the SAGCA was lost as it was felt that the process may not be sustainable without government ownership and support. However, with the change of leadership at the Mission Directorate level in 2010, the efforts of SAGCA regained momentum.
1. Gaon Swashtya Samikhya is an expression in the Odiya language which loosely translates to Village Health Review.
2. NRHM is a common platform for delivery of public health services in rural India.
3. The Panchayati Raj Institutions or PRI are the local self government institutions at the village, subdistrict and district levels comprising of locally elected representatives.
The term community monitoring had been changed to community action during the course of implementation of Phase-I project to involve all stakeholders and for imbibing a shared perspective of fact finding rather than fault finding for improved planning and implementation of the health programmes in the community.
Gaon Swasthya Samikhya-(Community Action –Phase-II)
The term community monitoring had been changed to community action during the course of implementation of Phase-I project to involve all stakeholders and for imbibing a shared perspective of fact finding rather than fault finding for improved planning and implementation of the health programmes in the community. To bring in further innovations the programme is proposed to be renamed as Gaon Swasthya Samikhya (GSS). A concept note on the modified operational guideline was presented before the SAGCA on 10th June 2010 with the chairmanship of Dr. Pramod Meherda, IAS, Mission Director, NRHM. To bring in improvement in the draft operational guideline different committees were constituted. The SAGCA was also restructured and formed.
The term community monitoring had been changed to community action during the course of implementation of Phase-I project to involve all stakeholders and for imbibing a shared perspective of fact finding rather than fault finding for improved planning and implementation of the health programmes in the community. To bring in further innovations the programme is proposed to be renamed as Gaon Swasthya Samikhya (GSS). A concept note on the modified operational guideline was presented before the SAGCA on 10th June 2010 with the chairmanship of Dr. Pramod Meherda, IAS, Mission Director, NRHM. To bring in improvement in the draft operational guideline different committees were constituted. The SAGCA was also restructured and formed.
|
The Advisory Group for Community Action (AGCA) was constituted under the chairmanship of Mission Director, NRHM, to provide technical support for the implementation of community monitoring during the pilot phase. The same group was notified to provide technical support for the implementation of GSS. The group is headed by Mission Director, NRHM and consists of directors from health, women and child development, panchayati raj and rural development departments and members from civil society organisations.
Roles and responsibilities of AGCA
|
- To support preparation of required module and materials; including providing support as resource person for conducting meeting and capacity building programmes.
- To undertake field visit to districts and blocks to provide supportive supervision at different levels for the effective implementation of programmes.
- To coordinate among different departments and other stakeholders to strengthen inter-sectoral convergence.
- To develop criteria for selection of nodal agencies at the district and block level. In addition, provide required support to the nodal agencies for field implementation of the programme.
|
|
|
Process of formulating Gaon Swasthya Samikhya programme
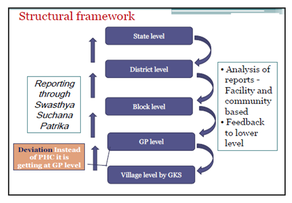
the process is to start from the village where gaon kalyan samitis (GKS) have been formed at the revenue village level to be a platform to address the health issues and promote community level action. GKS members meet every month to discuss the health issues of the village. It is proposed to use this opportunity to integrate the discussion on birth and death in the meeting, leading to further analysis of causes, service availability and utilisation, and identify action points at different levels that could prevent such deaths. This will be linked to reporting and analysis on the delivery, quality, availability, and reach of the services at the village/gram panchayat (GP), block and district level and taking appropriate actions for required service delivery. Focus being fact finding not fault finding and moving from event to service and evidence based analysis and reporting. |
|
Issue 3, July 2013
Page 18
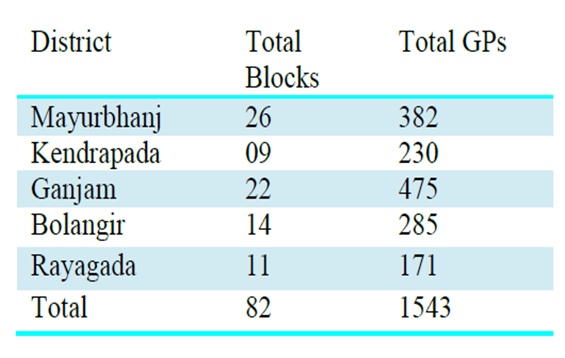
Currently under GSS, five districts, 82 blocks and 1543 GPs have been taken as initial implementation of activities. However, there is a felt need of transforming community action in more number of districts. The year 2013-14 will be targeted to 10 districts, 169 blocks, 15,000 GPs and 27,000 villages for GSS programme implementation.
Page 18
Currently under GSS, five districts, 82 blocks and 1543 GPs have been taken as initial implementation of activities. However, there is a felt need of transforming community action in more number of districts. The year 2013-14 will be targeted to 10 districts, 169 blocks, 15,000 GPs and 27,000 villages for GSS programme implementation.
Current status of implementation of Gaon Swasthya Samikhya in Odisha
The implementation process of GSS programme in the state of Odisha has been robustly planned and started from 2012. With the proactive role by AGCA Odisha, the process has been rolled out with the support of NRHM. Five districts, 82 blocks and 1543 villages have been taken to carry out GSS programme in the state.
To implement the entire process, Human Development Foundation (HDF), Bhubaneswar a state level civil society organisation has been assigned as nodal agency to carry out the “Swasthya Samikhya” in the state.
Progress at a glance of Gaon Swasthya Samikhya programme implementation in Odisha
The state training of trainers for the GSS programme was organised for key stakeholders to discuss about relevance, need and perspective of community monitoring, role of GKS promoting the Swasthya Samikhya programme, health and socialdeterminants of health, formation and role of swasthya samikhya samitis at district, block and GP Level. GSS programme was launched by the Chief Minister of Odisha Shri. Naveen Patnaik at Karanjia, Mayurbhanj on 2nd March, 2013
Conclusion and Way Forward
Involvement of community in public health care is a critical task as it needs to interlink convergence and involve key stakeholders from all related fields of health. Though the policy document of NRHM lays emphasis upon community involvement and participation in health care but achievement is very poor. Health for all will be dream for all as long as community ownership will not be impulsively sprouted. The community based monitoring has initiated the process of empowering the community in Odisha, but still, all districts have not been covered under the CBM process. Currently under GSS, five districts, 82 blocks and 1543 GPs have been taken as initial implementation of activities. However, there is a felt need of transforming community action in more number of districts. The year 2013-14 will be targeted to 10 districts, 169 blocks, 15,000 GPs and 27,000 villages for GSS programme implementation. To organise activities from village level to state level is hard task but with proper proactive planning from divergent levels, the goal of NRHM “A community led health care system where community will plan, manage and utilise the health services” can be achieved.
The implementation process of GSS programme in the state of Odisha has been robustly planned and started from 2012. With the proactive role by AGCA Odisha, the process has been rolled out with the support of NRHM. Five districts, 82 blocks and 1543 villages have been taken to carry out GSS programme in the state.
To implement the entire process, Human Development Foundation (HDF), Bhubaneswar a state level civil society organisation has been assigned as nodal agency to carry out the “Swasthya Samikhya” in the state.
Progress at a glance of Gaon Swasthya Samikhya programme implementation in Odisha
- Based on the learning of the first phase of community monitoring activity implementation, subsequent discussions and consultations, a detailed operational guideline, posters, brochure and information booklets (Suchana Patrika) have been prepared. The Suchana Patrika has been developed based on several indicators like infant death, maternal death, their cause, steps taken by GKS, immunisation status and sanitation, etc.
- For the effective implementation of the programme, review committees (Swasthya Samikhya Samitis) have been constituted at the village, block, district and state level. At the state level, a review committee has been constituted comprising different government functionaries as its members.
- To strengthen GSS, the district level advocacy workshops on GSS have been organised. The prime objectives for organising the workshop was to sensitise the participants about the programme.
- To carry out “Swasthya Samikhya” (community monitoring) process at the block and district level, NGO selection process is underway. A training manual has been developed and designed to operationalise the modus operandi for implementation of GSS at the grassroots level.
The state training of trainers for the GSS programme was organised for key stakeholders to discuss about relevance, need and perspective of community monitoring, role of GKS promoting the Swasthya Samikhya programme, health and socialdeterminants of health, formation and role of swasthya samikhya samitis at district, block and GP Level. GSS programme was launched by the Chief Minister of Odisha Shri. Naveen Patnaik at Karanjia, Mayurbhanj on 2nd March, 2013
Conclusion and Way Forward
Involvement of community in public health care is a critical task as it needs to interlink convergence and involve key stakeholders from all related fields of health. Though the policy document of NRHM lays emphasis upon community involvement and participation in health care but achievement is very poor. Health for all will be dream for all as long as community ownership will not be impulsively sprouted. The community based monitoring has initiated the process of empowering the community in Odisha, but still, all districts have not been covered under the CBM process. Currently under GSS, five districts, 82 blocks and 1543 GPs have been taken as initial implementation of activities. However, there is a felt need of transforming community action in more number of districts. The year 2013-14 will be targeted to 10 districts, 169 blocks, 15,000 GPs and 27,000 villages for GSS programme implementation. To organise activities from village level to state level is hard task but with proper proactive planning from divergent levels, the goal of NRHM “A community led health care system where community will plan, manage and utilise the health services” can be achieved.

|
SHARE YOUR FEEDBACK
|

|

|

|

|

ABOUT AUTHORS
Sudarshan Das is a development thinker, columnist, leader and institution builder. He started his career as a lecturer in sociology and has more than a decade of research and academic experience. Mr. Das has held various positions of responsibility including Director, Centre for Social Development; Dean, Student Welfare; and Registrar at KIIT University. He has been associated in various capacities in many civil society organisations in the country. Mr. Das is a regular columnist in the daily Oriya newspapers, The Samband and The Pragatibadi and many other journals and periodicals.
Sudarshan Das is a development thinker, columnist, leader and institution builder. He started his career as a lecturer in sociology and has more than a decade of research and academic experience. Mr. Das has held various positions of responsibility including Director, Centre for Social Development; Dean, Student Welfare; and Registrar at KIIT University. He has been associated in various capacities in many civil society organisations in the country. Mr. Das is a regular columnist in the daily Oriya newspapers, The Samband and The Pragatibadi and many other journals and periodicals.
